What it is
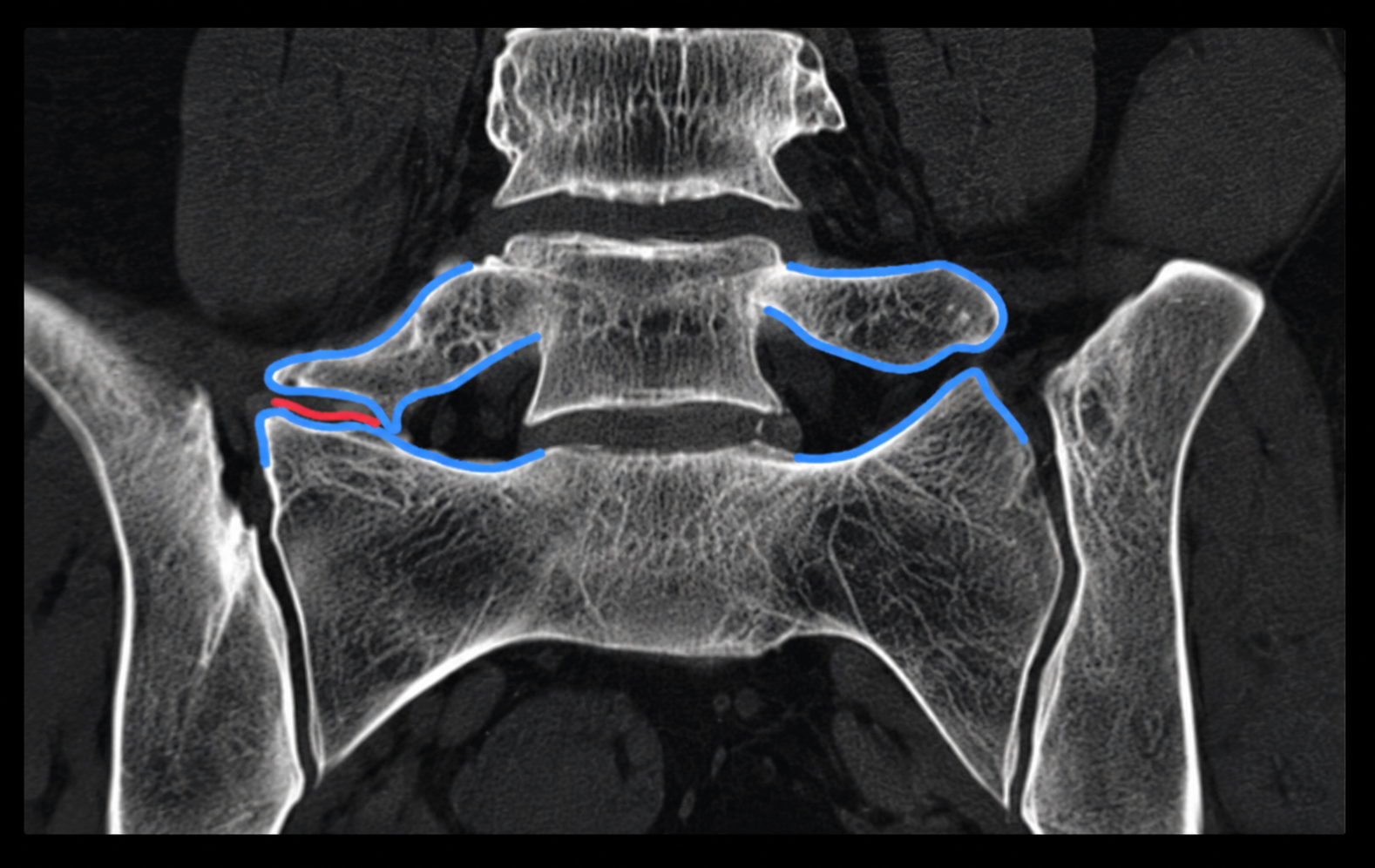
Bertolotti's syndrome is caused by an enlarged, elongated transverse process at the L5 vertebra that forms a pseudo-joint with the top of the sacrum or iliac wing. This anomaly is a transitional variation of the lumbosacral junction, present in a small proportion of the population. The abnormal joint creates a mechanical pain source that is poorly responsive to standard back pain treatments, leading to years of misdiagnosis for many patients.